
This Key Event Relationship is licensed under the Creative Commons BY-SA license. This license allows reusers to distribute, remix, adapt, and build upon the material in any medium or format, so long as attribution is given to the creator. The license allows for commercial use. If you remix, adapt, or build upon the material, you must license the modified material under identical terms.
Relationship: 3350
Title
Decrease, circulating testosterone levels leads to Hypospadias
Upstream event
Downstream event
Key Event Relationship Overview
AOPs Referencing Relationship
| AOP Name | Adjacency | Weight of Evidence | Quantitative Understanding | Point of Contact | Author Status | OECD Status |
|---|---|---|---|---|---|---|
| Decreased testosterone synthesis leading to hypospadias in male (mammalian) offspring | non-adjacent | Low | Terje Svingen (send email) | Under development: Not open for comment. Do not cite |
Taxonomic Applicability
Sex Applicability
| Sex | Evidence |
|---|---|
| Male | High |
Life Stage Applicability
| Term | Evidence |
|---|---|
| Foetal | High |
Key Event Relationship Description
This non-adjacent KER describes a decrease in circulating testosterone (often measured in serum or plasma) during the fetal male masculinization programming window leading to hypospadias in male offspring.
In male mammals, testosterone along with its more potent derivative dihydrotestosterone (DHT) drives male reproductive differentiation. Produced by the fetal testes, testosterone is transported through blood to the peripheral reproductive tissues to bind the androgen receptor (AR) or be converted to DHT (Murashima et al., 2015). Activation of AR in the genital tubercle directs its differentiation to a penis, and failure of this differentiation can lead to malformations, including hypospadias where the urethra terminates on the underside of the penis. The androgen programming of the genital tubercle is largely (but not fully) constrained to the masculinization programming window (gestational days (GD) 16-20 in rats, presumably gestational weeks (GW) 8-14 in humans), when circulating testosterone levels are high (Sharpe, 2020; Welsh et al., 2014).
A decrease in circulating testosterone levels in the masculinization programming window can thus disrupt penis differentiation and cause hypospadias.
Evidence Collection Strategy
A systematic approach (fig. 1, 2tlnravl4v_KER_3350_Figure_1.png (1288×281)) was used to collect evidence based on the methodology described in (Holmer et al., 2024). The evidence collection for this KER was done concurrently with the evidence collection for KER 3488 ‘decrease, intratesticular testosterone leads to hypospadias, for which the same search string was used.
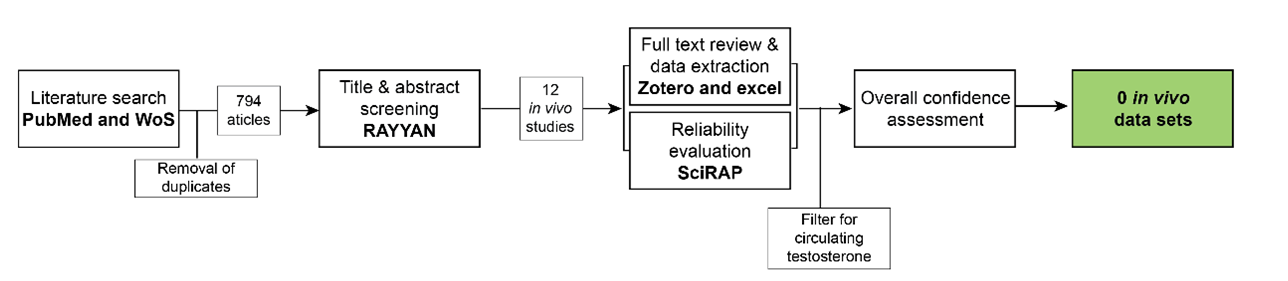{kind=link}
Search strategy
Search strings were synthesized for PubMed and Web of Science Core Collection based on the review question ‘Does decreased testosterone during fetal development lead to hypospadias in male mammals?’
Search string in PubMed: ("testosterone*") AND ("genital malformation*" OR "hypospadias"[MeSH terms] OR “hypospadia*”)
Search string in Web of Science Core Collection: ("testosterone*”) AND ("hypospadia*" OR "genital malformation*")
Title & abstract screening:
Retrieved articles were screened in the online tool RAYYAN https://www.rayyan.ai/ After removal of duplicates, the titles and abstracts of the remaining 793 articles were screened according to pre-defined inclusion and exclusion criteria:
Inclusion criteria:
- In vivo studies in male mammals where fetal testosterone is reduced and hypospadias is evaluated*
- Mechanistic reviews on hypospadias
- Epidemiologic and human case studies with measurement of testosterone levels and hypospadias as an outcome. Chromosomal abnormalities were excluded from human case studies.
- In vitro, ex vivo, and in vivo mechanistic studies on hypospadias or testosterone production
- Non-clinical reviews on hypospadias
Exclusion criteria:
- Papers not in English
- Abstracts and other non-full text publications
*In cases where this criterion could not be determined by reading the abstract, the studies were included for full text review.
Full text review, data extraction and reliability evaluation of animal studies:
For the in vivo studies, full text papers were reviewed using the same exclusion criteria as in the title & abstract screening, and data were extracted from the included papers into an Excel template. In parallel, methodological reliability was assessed using the online tool Science in Risk Assessment and Policy (SciRAP; http://www.scirap.org, see Appendix 1, 3357003l2q_KER_3350__appendix_1.pdf. Based on the SciRAP evaluations, animal studies were assigned a reliability category using the principles outlined in Table 1. Studies were divided into different datasets, if multiple different chemicals, different exposure windows, or different time points of measurement of hypospadias were included.
Moreover, as this KER was developed in parallel with several other KERs for other androgen-sensitive male reproductive endpoints (nipple retention and anogenital distance), three additional studies reporting on hypospadias, but not retrieved by the literature search for this KER, were also data-extracted and evaluated for reliability.
The collected data were filtered to only include data sets measuring circulating testosterone, either in plasma or serum. Mixture studies were excluded to avoid different chemicals having different modes-of-action.
Overall assessment of empirical evidence was performed following the guidelines in the AOP handbook.
Table 1 Principles for translation SciRAP evaluations into reliability categories.
|
Reliability Category |
Principles for Categorization |
|
1.Reliable without restriction |
SciRAP methodological quality Score > 80 and all key criteriaa are “Fulfilled” and there are no deficiencies in the non-key criteria that might affect study reliability. |
|
2. Reliable with restriction |
SciRAP methodological quality Score > 65 and one or several of the key criteria are “Partially Fulfilled” or there are minor deficiencies in the non-key criteria that might affect study reliability. |
|
3. Not reliable |
SciRAP methodological quality Score < 65 or one or several of the key criteria are “Not Fulfilled” or there are major deficiencies in the non-key criteria that affect study reliability. |
|
4. Not assignable |
Two or more of the key criteria are “Not Determined” |
aKey criteria were criteria judged as specifically critical for reliability of the data for this KER and were determined a priori. The key criteria for this data collection are outlined in Appendix 1, 3357003l2q_KER_3350__appendix_1.pdf..
Human studies
Studies in humans were regarded as supporting evidence, and study quality was not systematically evaluated. All studies were assessed for any major errors in study design or interpretation. For this KER, supporting evidence are case studies of humans with hypospadias and a reduction in circulating testosterone levels.
Evidence Supporting this KER
Biological Plausibility
The biological plausibility for this KER is judged to be high given the canonical biological knowledge on normal reproductive development.
Sexual differentiation in males, the external genitalia, is initiated and programmed in fetal life. Once the testes have formed, they synthesize testosterone through the steroidogenesis pathway and secrete it into circulation. Testosterone is transported in the blood either as free testosterone or bound to albumin or sex-hormone binding globulin. Testosterone is produced from around GD15 in fetal rats and GW8 in humans, which is also the onset of when testosterone levels can be measured in circulation. In peripheral tissues, testosterone can be converted to the more potent androgen DHT by the enzyme 5α-reductase. Both DHT and testosterone bind and activate the AR to program fetal tissues to differentiate along the male pathway (Murashima et al., 2015; Trost & Mulhall, 2016; Welsh et al., 2014).
The genital tubercle is the bipotential structure that upon hormonal cues differentiates to either penis or clitoris. Both human and rodent genital tubercles express AR (C. M. Amato & Yao, 2021; Baskin et al., 2020). Upon activation of AR, the genital tubercle differentiates to a penis by elongation and formation of a central urethra which terminates at the tip of the penis (C. Amato et al., 2022). The programming of the genital tubercle happens in the masculinization programming window (GD16-20 in rats, GW8-14 in humans) (Welsh et al., 2014), although elongation and growth of the penis is also programmed later, at least in rats (Welsh et al., 2008). Hypospadias is one of the most common genital malformations caused by disruptions to penis development (Baskin & Ebbers, 2006; Yu et al., 2019).
Given the dependency of testosterone for penis differentiation, either through direct AR activation or conversion to DHT, it is plausible that a decrease in circulating levels of testosterone will cause hypospadias.
Empirical Evidence
The empirical evidence from studies in animals for this KER is judged as low overall.
From the data collection, two toxicity studies were extracted which reported a decrease in circulating testosterone levels in fetal male rats and measured hypospadias in male offspring. However, both studies were classified as not reliable (category 3). Due to the lack of any reliable studies for this KER, the evidence from the two unreliable data sets is included, although they are considered weak evidence for the KER.
In this first study (Li et al., 2017), rats were exposed to 0 or 750 mg/kg bw/day dibutylphthalate (DBP) from GD13-18. At GD19, serum testosterone and hypospadias were evaluated. At this stage, 43.6% of males exposed to DBP had hypospadias upon examination. In the hypospadias group, serum testosterone levels were 3.93 nmol/mL compared to 15.74 nmol/mL in control male rats. In exposed rats without hypospadias, serum testosterone levels were 5.89 nmol/mL. This study was categorized as unreliable, mainly due to the evaluation of hypospadias being on GD19, a timepoint at which the penis is not finished differentiating. This poses an uncertainty, in particular regarding the frequency of hypospadias reported in the exposure group.
The second study (Vo et al., 2009) was considered unreliable due to a too low reliability score (64.7) with some key information not reported. In this study, no major deficiencies were noted. Rats were exposed to 0, 10, 100, or 500 mg/kg bw/day diethylhexylphthalate (DEHP) from GD11-21. At GD21, plasma testosterone levels were reduced in males in the highest exposure group (0.53 ±0.16 ng/mL) compared to control males (1.56 ±0.84 ng/mL), but not in the other dose groups. Hypospadias was evaluated in male offspring at postnatalday 63, and hypospadias was registered in 23/100 male pups exposed in utero to 500 mg/kg bw/day. There was no hypospadias in the other groups.
Supporting human case studies
Supporting this KER are case studies of humans with hypospadias and a reduction in circulating testosterone levels.
Studies extracted from the literature search are summarized in Table 2.
Table 2: Human case studies of hypospadias with reductions in circulating testosterone levels (measured postnatally).
|
Case |
Effect on upstream event (circulating testosterone) |
Effect on downstream event hypospadias |
Reference |
|
Subject with mutation in HSD17B3 |
Six weeks: 2.5 nmol/L (reference range 0-6.5 nmol/L) 10 years: 3.6 nmol/L (reference range: 9.0-31.0 nmol/L) |
Ambiguous genitalia / hypospadias |
(Al-Sinani et al., 2015) |
|
7 subjects (0-2 years) with perineal or penoscrotal hypospadias |
Testosterone levels < 2 ng/mL after hCG stimulation. In 2 subjects, testosterone response returned to normal |
Perineal or penoscrotal hypospadias |
(Allen & Griffin, 1984) |
|
18-year old subject |
Basal testosterone levels 0.8 ng/mL (normal range 2.8-18.5 ng/mL). hCG stimulated testosterone levels: 0.9 ng/mL |
Perineal hypospadias |
(Ammini et al., 1997) |
|
2 subjects (15 and 12 years old) with INHA mutations |
Testosterone levels: 0.68 and 1.48 ng/mL (normal range 2.4-9.5 ng/mL) |
Hypospadias |
(Arslan Ates et al., 2022) |
|
8 subjects |
hCG-stimulated testosterone levels in childhood < 3 ng/mL |
Proximal hypospadias |
(Blanc et al., 2011) |
|
Subject with unilateral vanishing testes syndrome |
Insufficient testosterone syndrome after hCG stimulation |
Severe hypospadias |
(Boehmer et al., 2001) |
|
Newborn subject |
Testosterone levels: 18 ng/dL (normal range 60-570 ng/dL) |
Perineal hypospadias |
(Dean et al., 1984) |
|
13 subjects (1/2-10 years) |
Low basal testosterone (0-0.34 ng/mL) and poor or absent response to hCG stimulation |
Penoscrotal, scrotal or perineal hypospadias |
(Iyengar et al., 1986) |
|
5 year old subject |
Testosterone response to hCG stimulation: 12-17 ng/dL (normal values 667 ng/dL) |
Perineal hypospadias |
(Kaufman et al., 1983) |
|
Three subjects (0-4 years) with NR5A1 mutations |
Low testosterone levels (basal 0.05-0.4 ng/mL; hCG-stimulated 0.58-0.9 ng/mL) |
Penoscrotal hypospadias |
(Köhler et al., 2009) |
|
Subject with mutation in the gene encoding LH receptor |
No response to hCG stimulation (0.05 ng/mL) |
Severe hypospadias |
(Misrahi et al., 1997) |
|
2 subjects evaluated at puberty |
Decreased testosterone |
One mild and one severe hypospadias |
(Moriya et al., 2010) |
|
10-year old subject with HSD17B3 mutation |
Baseline testosterone: 59.2 ng/dL, hCG stimulated testosterone: 139.9 ng/dL (no reference values given) |
Hypospadias |
(Neocleous et al., 2012) |
|
24-year old subject |
Testosterone levels 0.3-0.4 µg/100 mL (no reference values given) |
Severe hypospadias |
(New, 1970) |
|
6-year old subject |
Low testosterone response to hCG stimulation |
Perineal hypospadias |
(Pang et al., 1983) |
|
Infant subject with CYP11A1 mutation |
Low testosterone response to hCG stimulation (0.7 nmol/L), but normal serum testosterone |
Penoscrotal hypospadias |
(Parajes et al., 2012) |
|
Infant subject with LHGCR mutation |
At birth: 0.24 ng/mL 10 weeks: 0.06 ng/mL 2 years: 0.02 ng/mL (normal range 0.03-0.52 ng/mL). No response in testosterone levels after hCG stimulation |
Perineal hypospadias |
(Richard et al., 2011) |
|
Subject with WT1 mutation |
Low testosterone levels: 1.02 ng/mL (no reference values given) |
Glandular hypospadias |
(Schumacher et al., 2008) |
|
Subject with NR5A1 mutation |
12 hours old: 0.9 nmol/L (low) 2 days old: <0.1 nmol/L (normal) In later years, slight increase at 9 years, then normal or decreased levels during teen years |
Perineal hypospadias |
(Teoli et al., 2023) |
|
Newborn with GPC3 mutation (Simpson-Golabi-Behmel syndrome) |
1 day old: 42 ng/dL (reference range 75-400 ng/dL) 20 days old: 55 ng/dL (reference range: 60-400 ng/dL) 26 days old after hCG stimulation: 130 ng/dL (reference range: 60-400 ng/dL) |
Midshaft hypospadias |
(Villarreal et al., 2013) |
|
Subject with MAMLD1 mutation |
2 months: 49 ng/dL (reference level: 196 ng/dL) |
Hypospadias |
(Yeste et al., 2022) |
Dose concordance
Dose concordance cannot be informed from the two in vivo studies, although the study (Vo et al., 2009) does not argue against dose concordance as the upstream and downstream events were measured at the same dose of DEHP.
Temporal concordance
Iin (Vo et al., 2009) plasma testosterone levels were decreased at GD21, while hypospadias was diagnosed in adult rats, long after exposure was ceased. In (Li et al., 2017), hypospadias and testosterone levels were assessed/measured at the same time point (GD19), however this is known not to be an optimal time point for hypospadias diagnosis in rats as the penis is not finished developing.
Incidence concordance
The study with DBP supports incidence concordance, because the non-hypospadiac rats exposed to DBP also had lower serum testosterone levels compared to control rats at GD19 (Li et al., 2017). This is however only weak evidence, as hypospadias was not evaluated at an optimal time point.
Uncertainties and Inconsistencies
The uncertainties of the two in vivo studies have been discussed. Both were classified as unreliable in the evaluation of methodological reliability. Of the two studies, the study by (Li et al., 2017) is considered most uncertain due to the timepoint of hypospadias assessment. A study with in utero exposure to an 5α-reductase inhibitor disrupted genital tubercle development at GD19, but hypospadias was not observed at postnatal day 90, indicating that assessment prior to birth may not be true indications of postnatal outcomes (Iguchi et al., 1991). The deficiencies in (Vo et al., 2009) are less severe but overall poses an uncertainty to the study due to missing key information about study design.
The uncertainties in the human evidence mainly pertains to the fact that testosterone levels were not measured during fetal life but in newborn or juvenile males. Given that most cases involve genetic mutations, which occur early in embryonic life, it is highly likely that the effects of mutations on testosterone levels manifest early in fetal life. Another uncertainty with the human cases which include mutations is that it cannot be excluded that the hypospadias phenotype is caused by the low testosterone levels and not directly by genetic mutation.
Another uncertainty for this KER from the literature is the observation that humans with 5α-reductase deficiency have hypospadias due to low DHT levels despite normal or higher testosterone levels (Mendonca et al., 1996). This indicates that the effects of low testosterone may be more through reduced conversion to DHT than due to a direct loss of testosterone action on AR. To this, there is also the existence of a “backdoor pathway” to DHT in humans. This pathway in peripheral tissues (i.e. not testes) can circumvent testosterone as a precursor for DHT by synthesis of DHT is from reduction of androsterone by 17β-HSD (Miller & Auchus, 2019). This would create the possibility that testosterone is not required for DHT production and ultimately AR activation.
Known modulating factors
There are no known modulating factors for this KER.
Quantitative Understanding of the Linkage
The quantitative understanding of this KER is low.
Response-response Relationship
Time-scale
The time-scale for this KER depends on species but is likely weeks. Testosterone is secreted from around GW8 in humans (GD16 in rats), marking the beginning of the masculinization programming window and programming of the genital tubercle. Hypospadias is diagnosed at birth in humans (Yu et al., 2019) and can also be observed at birth in rodents, but as development of the penis continues after birth in rodents, hypospadias may be more optimally evaluated later in juvenile or adult male rats (Schlomer et al., 2013; Sinclair et al., 2017).
Known Feedforward/Feedback loops influencing this KER
Local disruption of AR activation in the genital tubercle irreversibly disrupts development, so there are no known feedback/feedforward loops for this KER.
Domain of Applicability
Taxonomic applicability
Sexual differentiation of the penis is an androgen-driven process in mammals, and it is therefore biologically plausible that this KER is applicable to all mammals (Murashima et al., 2015). The empirical evidence in this KER provides support that hypospadias in humans is associated with reduced circulating testosterone levels in early life. The two in vivo studies included in the empirical evidence support the applicability to rats.
Sex applicability
The empirical evidence in this KER supports that reduced circulating testosterone is linked to hypospadias in males. Females do have circulating testosterone, but in much lower concentrations than males (Vesper et al., 2015). Moreover, the term hypospadias is mainly used for malformation of the male external genitalia.
Life stage applicability
The genital tubercle is programmed by the surge in androgen hormones during the masculinization programming window is (GD16-20 in rats and GW8-14 in humans ) (Sharpe, 2020; Welsh et al., 2014). In humans, the penis is fully formed at birth (Yu et al., 2019), while penis development continues postnatally around 20-25 days in rats and mice (Schlomer et al., 2013; Sinclair et al., 2017).
References
Allen, T., & Griffin, J. (1984). Endocrine studies in patients with advanced hypospadias. The Journal of Urology, 131(2), 310–314. https://doi.org/10.1016/s0022-5347(17)50360-2
Al-Sinani, A., Mula-Abed, W., Al-Kindi, M., Al-Kusaibi, G., Al-Azkawi, H., & Nahavandi, N. (2015). A Novel Mutation Causing 17-β-Hydroxysteroid Dehydrogenase Type 3 Deficiency in an Omani Child: First Case Report and Review of Literature. Oman Medical Journal, 30(2), 129–134. https://doi.org/10.5001/omj.2015.27
Amato, C., Fricke, A., Marella, S., Mogus, J., Bereman, M., & McCoy, K. (2022). An experimental evaluation of the efficacy of perinatal sulforaphane supplementation to decrease the incidence and severity of vinclozolin-induced hypospadias in the mouse model. Toxicology and Applied Pharmacology, 451, 116177. https://doi.org/10.1016/j.taap.2022.116177
Amato, C. M., & Yao, H. H.-C. (2021). Developmental and sexual dimorphic atlas of the prenatal mouse external genitalia at the single-cell level. Proceedings of the National Academy of Sciences of the United States of America, 118(25). https://doi.org/10.1073/pnas.2103856118
Ammini, A., Sharma, D., Gupta, R., Mohapatra, I., Kucheria, K., Kriplani, A., Takkar, D., Mitra, D., & Vijayaraghavan, M. (1997). Familial male pseudohermaphroditism. Indian Journal of Pediatrics, 64(3), 419–423. https://doi.org/10.1007/BF02845218
Arslan Ates, E., Eltan, M., Sahin, B., Gurpinar Tosun, G., Seven Menevse, T., Geckinli, B., Greenfield, A., Turan, S., Bereket, A., & Guran, T. (2022). Homozygosity for a novel INHA mutation in two male siblings with hypospadias, primary hypogonadism, and high-normal testicular volume. European Journal of Endocrinology, 186(5), K25–K31. https://doi.org/10.1530/EJE-21-1230
Baskin, L., Cao, M., Sinclair, A., Li, Y., Overland, M., Isaacson, D., & Cunha, G. R. (2020). Androgen and estrogen receptor expression in the developing human penis and clitoris. Differentiation; Research in Biological Diversity, 111, 41–59. https://doi.org/10.1016/j.diff.2019.08.005
Baskin, L., & Ebbers, M. (2006). Hypospadias: Anatomy, etiology, and technique. Journal of Pediatric Surgery, 41(3), 463–472. https://doi.org/10.1016/j.jpedsurg.2005.11.059
Blanc, T., Ayedi, A., El-Ghoneimi, A., Abdoul, H., Aigrain, Y., Paris, F., Sultan, C., Carel, J., & Léger, J. (2011). Testicular function and physical outcome in young adult males diagnosed with idiopathic 46 XY disorders of sex development during childhood. European Journal of Endocrinology, 165(6), 907–915. https://doi.org/10.1530/EJE-11-0588
Boehmer, A., Nijman, R., Lammers, B., de Coninck, S., Van Hemel, J., Themmen, A., Mureau, M., de Jong, F., Brinkmann, A., Niermeijer, M., & Drop, S. (2001). Etiological studies of severe or familial hypospadias. The Journal of Urology, 165(4), 1246–1254.
Dean, H., Shackleton, C., & Winter, J. (1984). Diagnosis and natural history of 17-hydroxylase deficiency in a newborn male. The Journal of Clinical Endocrinology and Metabolism, 59(3), 513–520. https://doi.org/10.1210/jcem-59-3-513
Holmer, M. L., Zilliacus, J., Draskau, M. K., Hlisníková, H., Beronius, A., & Svingen, T. (2024). Methodology for developing data-rich Key Event Relationships for Adverse Outcome Pathways exemplified by linking decreased androgen receptor activity with decreased anogenital distance. Reproductive Toxicology, 128, 108662. https://doi.org/10.1016/j.reprotox.2024.108662
Iguchi, T., Uesugi, Y., Takasugi, N., & Petrow, V. (1991). Quantitative analysis of the development of genital organs from the urogenital sinus of the fetal male mouse treated prenatally with a 5 alpha-reductase inhibitor. The Journal of Endocrinology, 128(3), 395–401. https://doi.org/10.1677/joe.0.1280395
Iyengar, J., Rohatgi, M., Menon, P., Mathews, A., Verma, I., & Bhargava, S. (1986). Clinical, cytogenetic & hormonal profile in extreme hypospadias with bilaterally descended testes. The Indian Journal of Medical Research, 83, 604–609.
Kaufman, F., Costin, G., Goebelsmann, U., Stanczyk, F., & Zachmann, M. (1983). Male pseudohermaphroditism due to 17,20-desmolase deficiency. The Journal of Clinical Endocrinology and Metabolism, 57(1), 32–36. https://doi.org/10.1210/jcem-57-1-32
Köhler, B., Lin, L., Mazen, I., Cetindag, C., Biebermann, H., Akkurt, I., Rossi, R., Hiort, O., Grüters, A., & Achermann, J. (2009). The spectrum of phenotypes associated with mutations in steroidogenic factor 1 (SF-1, NR5A1, Ad4BP) includes severe penoscrotal hypospadias in 46,XY males without adrenal insufficiency. European Journal of Endocrinology, 161(2), 237–242. https://doi.org/10.1530/EJE-09-0067
Li, X., Li, J., Zhang, Y., & Zhou, Y. (2017). Di-n-butyl phthalate induced hypospadias relates to autophagy in genital tubercle via the PI3K/Akt/mTOR pathway. Journal of Occupational Health, 59(1), 8–16. https://doi.org/10.1539/joh.16-0089-OA
Mendonca, B., Inacio, M., Costa, E., Arnhold, I., Silva, F., Nicolau, W., Bloise, W., Russel, D., & Wilson, J. (1996). Male pseudohermaphroditism due to steroid 5alpha-reductase 2 deficiency. Diagnosis, psychological evaluation, and management. Medicine, 75(2), 64–76. https://doi.org/10.1097/00005792-199603000-00003
Miller, W. L., & Auchus, R. J. (2019). The “backdoor pathway” of androgen synthesis in human male sexual development. PLoS Biology, 17(4), e3000198. https://doi.org/10.1371/journal.pbio.3000198
Misrahi, M., Meduri, G., Pissard, S., Bouvattier, C., Beau, I., Loosfelt, H., Jolivet, A., Rappaport, R., Milgrom, E., & Bougneres, P. (1997). Comparison of immunocytochemical and molecular features with the phenotype in a case of incomplete male pseudohermaphroditism associated with a mutation of the luteinizing hormone receptor. The Journal of Clinical Endocrinology and Metabolism, 82(7), 2159–2165. https://doi.org/10.1210/jcem.82.7.4039
Moriya, K., Mitsui, T., Tanaka, H., Nakamura, M., & Nonomura, K. (2010). Long-term outcome of pituitary-gonadal axis and gonadal growth in patients with hypospadias at puberty. The Journal of Urology, 184(4), 1610–1614. https://doi.org/10.1016/j.juro.2010.04.022
Murashima, A., Kishigami, S., Thomson, A., & Yamada, G. (2015). Androgens and mammalian male reproductive tract development. Biochimica et Biophysica Acta (BBA) - Gene Regulatory Mechanisms, 1849(2), 163–170. https://doi.org/10.1016/j.bbagrm.2014.05.020
Neocleous, V., Sismani, C., Shammas, C., Efstathiou, E., Alexandrou, A., Ioannides, M., Argyrou, M., Patsalis, P., Phylactou, L., & Skordis, N. (2012). Duplication of exons 3-10 of the HSD17B3 gene: A novel type of genetic defect underlying 17β-HSD-3 deficiency. GENE, 499(2), 250–255. https://doi.org/10.1016/j.gene.2012.03.031
New, M. (1970). Male pseudohermaphroditism due to 17 alpha-hydroxylase deficiency. The Journal of Clinical Investigation, 49(10), 1930–1941. https://doi.org/10.1172/JCI106412
Pang, S., Levine, L., Stoner, E., Opitz, J., Pollack, M., Dupont, B., & New, M. (1983). Nonsalt-losing congenital adrenal hyperplasia due to 3 beta-hydroxysteroid dehydrogenase deficiency with normal glomerulosa function. The Journal of Clinical Endocrinology and Metabolism, 56(4), 808–818. https://doi.org/10.1210/jcem-56-4-808
Parajes, S., Chan, A., But, W., Rose, I., Taylor, A., Dhir, V., Arlt, W., & Krone, N. (2012). Delayed diagnosis of adrenal insufficiency in a patient with severe penoscrotal hypospadias due to two novel P450 side-change cleavage enzyme (CYP11A1) mutations (p.R360W; p.R405X). European Journal of Endocrinology, 167(6), 881–885. https://doi.org/10.1530/EJE-12-0450
Richard, N., Leprince, C., Gruchy, N., Pigny, P., Andrieux, J., Mittre, H., Manouvrier, S., Lahlou, N., Weil, J., & Kottler, M. (2011). Identification by array-Comparative Genomic Hybridization (array-CGH) of a large deletion of luteinizing hormone receptor gene combined with a missense mutation in a patient diagnosed with a 46,XY disorder of sex development and application to prenatal diagnosis. Endocrine Journal, 58(9), 769–776. https://doi.org/10.1507/endocrj.k11e-119
Schlomer, B. J., Feretti, M., Rodriguez, E. J., Blaschko, S., Cunha, G., & Baskin, L. (2013). Sexual differentiation in the male and female mouse from days 0 to 21: A detailed and novel morphometric description. The Journal of Urology, 190(4 Suppl), 1610–1617. https://doi.org/10.1016/j.juro.2013.02.3198
Schumacher, V., Gueler, B., Looijeng, L., Becker, J., Amann, K., Engers, R., Dotsch, J., Stoop, H., Schulz, W., & Royer-Pokora, B. (2008). Characteristics of testicular dysgenesis syndrome and decreased expression of SRY and SOX9 in Frasier syndrome. Molecular Reproduction and Development, 75(9), 1484–1494. https://doi.org/10.1002/mrd.20889
Sharpe, R. (2020). Androgens and the masculinization programming window: Human-rodent differences. Biochemical Society Transactions, 48(4), 1725–1735. https://doi.org/10.1042/BST20200200
Sinclair, A., Cao, M., Pask, A., Baskin, L., & Cunha, G. (2017). Flutamide-induced hypospadias in rats: A critical assessment. Differentiation; Research in Biological Diversity, 94, 37–57. https://doi.org/10.1016/j.diff.2016.12.001
Teoli, J., Mallet, D., Renault, L., Gay, C., Labrune, E., Bretone, P., Giscard D’Estaing, S., Cuzin, B., Dijoud, F., Roucher-Boulez, F., & Plotton, I. (2023). Case Report: Longitudinal follow-up and testicular sperm extraction in a patient with a pathogenic NR5A1 (SF-1) frameshift variant: P.(Phe70Serfs*5). Frontiers in Endocrinology, 14, 1171822. https://doi.org/10.3389/fendo.2023.1171822
Trost, L. W., & Mulhall, J. P. (2016). Challenges in Testosterone Measurement, Data Interpretation, and Methodological Appraisal of Interventional Trials. The Journal of Sexual Medicine, 13(7), 1029–1046. https://doi.org/10.1016/j.jsxm.2016.04.068
Vesper, H. W., Wang, Y., Vidal, M., Botelho, J. C., & Caudill, S. P. (2015). Serum Total Testosterone Concentrations in the US Household Population from the NHANES 2011-2012 Study Population. Clinical Chemisty, 61(12), 1495–1504. https://doi.org/10.1373/clinchem.2015.245969
Villarreal, D., Villarreal, H., Paez, A., Peppas, D., Lynch, J., Roeder, E., & Powers, G. (2013). A Patient With a Unique Frameshift Mutation in GPC3, Causing Simpson-Golabi-Behmel Syndrome, Presenting With Craniosynostosis, Penoscrotal Hypospadias, and a Large Prostatic Utricle. AMERICAN JOURNAL OF MEDICAL GENETICS PART A, 161(12), 3121–3125. https://doi.org/10.1002/ajmg.a.36086
Vo, T., Jung, E., Dang, V., Jung, K., Baek, J., Choi, K., & Jeung, E. (2009). Differential effects of flutamide and di-(2-ethylhexyl) phthalate on male reproductive organs in a rat model. The Journal of Reproduction and Development, 55(4), 400–411. https://doi.org/10.1262/jrd.20220
Welsh, M., Saunders, P., Fisken, M., Scott, H., Hutchison, G., Smith, L., & Sharpe, R. (2008). Identification in rats of a programming window for reproductive tract masculinization, disruption of which leads to hypospadias and cryptorchidism. The Journal of Clinical Investigation, 118(4), 1479–1490. https://doi.org/10.1172/JCI34241
Welsh, M., Suzuki, H., & Yamada, G. (2014). The masculinization programming window. Endocrine Development, 27, 17–27. https://doi.org/10.1159/000363609
Yeste, D., Aguilar-Riera, C., Canestrino, G., Fernández-Alvarez, P., Clemente, M., & Camats-Tarruella, N. (2022). A New MAMLD1 Variant in an Infant With Microphallus and Hypospadias With Hormonal Pattern Suggesting Partial Hypogonadotropic Hypogonadism-Case Report. Frontiers in Endocrinology, 13, 884107. https://doi.org/10.3389/fendo.2022.884107
Yu, X., Nassar, N., Mastroiacovo, P., Canfield, M., Groisman, B., Bermejo-Sánchez, E., Ritvanen, A., Kiuru-Kuhlefelt, S., Benavides, A., Sipek, A., Pierini, A., Bianchi, F., Källén, K., Gatt, M., Morgan, M., Tucker, D., Canessa, M. A., Gajardo, R., Mutchinick, O. M., … Agopian, A. J. (2019). Hypospadias Prevalence and Trends in International Birth Defect Surveillance Systems, 1980-2010. European Urology, 76(4), 482–490. https://doi.org/10.1016/j.eururo.2019.06.027